Written by a CuraCore Veterinary Medical Acupuncture course graduate. Signed release obtained from client/author. 3D2019005
Abstract
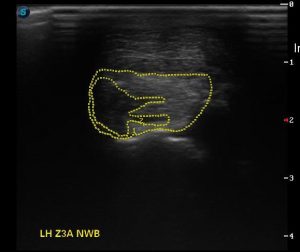
Walter, 15.1 hand, 3.5 year old Friesian Appaloosa gelding, suffered gradual onset, alternating left and right hind-limb lameness when started training under saddle in the winter of 2018. Diagnostic imaging of bilateral stifles and distal hind limbs were performed, which lead to a diagnosis of suspected Degenerative Suspensory Ligament Desmitis (DSLD) via ultrasonography and possible bilateral patellar lesions via radiography in March 2018. Acupuncture combined with massage techniques began in April 2018 in attempt to enhance analgesia, decrease inflammation and improve healing. Throughout 5 months of treatment, Walter’s hind limb lameness fluctuated from a 2/5 to a 1/5 on the American Association of Equine Veterinarian’s lameness scale (Figure 1), but his overall body soreness, improved significantly.
History and Presentation
Walter is a 15.1 hand, 3.5 year old, black, Friesian Appaloosa gelding that is being evaluated for bilateral hind-limb lameness. He is owned by a veterinarian whose practice focuses on equine, canine and feline patients. His owner is also certified in equine and small animal chiropractic. Ownership was signed over to his current owner due to severe malnutrition as a yearling. He was treated aggressively for severe hypoproteinemia over a course of one month. His treatment included 3 high albumin plasma transfusions. Walter seemed to recover without issue after initial treatment and was then pastured until the age of 3, when he was put into a training program to be a riding horse. Walter was ridden in an indoor arena with soft footing. He began sound in the walk and trot, but his trainer immediately noticed weakness in the canter. His weakness progressed to a 1/5- 2/5 lameness alternating between the right and left hind limbs, accompanied by significant bilateral stifle effusion, more pronounced in the right stifle. Walter’s under saddle training was put on hold and he was stall rested with 20 minutes of turn-out in the indoor arena daily. His owner performed chiropractic adjustments, myofascial release and two non-steroidal anti-inflammatory trials, but did not note any improvement in lameness. Radiographs of bilateral stifles were performed and reviewed by an equine surgeon, who suspected bilateral patellar lesions and recommended arthroscopy, but warned owner that Walter may still be lame after surgery. Walter was then started on and finished a 7 dose regiment of Adequan (polysulfated glycosaminoglycan), but he proceeded to get significantly more lame over the next few weeks. He became a 3/5 lame on his right hind and a 2/5 lame on his left hind when under saddle. His owner then scheduled an appointment for a full lameness work-up, diagnostic imaging and possible arthroscopic surgery. Lameness examination on this day showed moderate fetlock drop on the pavement, and tender suspensory ligaments on palpation, therefore ultrasound of bilateral distal hind limbs was performed. Ultrasound revealed bilateral suspensory ligament lesions consistent with DSLD (Figure 2). At this time, his owner elected to start aggressive treatment /management of DSLD. Walter was continued on stall rest with 20 minutes of daily walking/arena turn-out. His farrier applied Grand Circuit suspensory shoes on bilateral hind hooves to elevate the heal and off-load the suspensory ligaments. He received weekly shockwave treatments for 5 weeks to bilateral suspensory ligaments and bilateral patellar ligaments and was put on a 14 day course of Prednisone. He currently receives 3 grams of Jing Tang Ligament formula twice daily and is on Previcox (cycooxygenase-2 selective non-steroidal anti-inflammatory) once daily. His nutrition includes grass hay, Tribute Kalm N Ez grain and Vitamin E supplementation.
Despite aggressive multi-modal treatment of Walter’s condition, his owner did not appreciate any significant improvement in lameness and she found that Walter’s temperament was becoming sour and he was becoming body sore. It was at this time, in April 2019 that I was asked to perform acupuncture on Walter for its many beneficial properties, including, analgesic, anti-inflammatory and parasympathetic modulation.
Physical Examination and Clinical Assessments
All vital signs were within normal limits.
Neurologic examination: No neurologic deficits appreciated. When observed in his stall, Walter has appropriate mentation. He is bright, alert and responsive and shows appropriate responsiveness to normal stimuli. He has an appropriate menace and palpebral reflex, eye position is normal and pupils are equal size and reactive to light. When Walter was approached and a treat was offered, his ears turned forward, his muzzle and lips wiggled and he appropriately took the treat with his teeth, chewed it and swallowed it, all of which are indicators of appropriately functioning muscles of mastication, muscles of facial expression and an appropriate gag reflex. When walked out of his stall, Walter has appropriate foot fall and placement in all four limbs. Tail tone anal tone are normal. Cervicofacial, cutaneous trunci and peri-anal reflex are intact.
Gait assessment (performed on hard ground)/Lameness exam: When asked to pick up his feet, Walter willingly picks up bilateral front feet, but is heavy/slow to pick up bilateral back feet, and when he does lift them, it is done so with rapid/abrupt hyperflexion of his hock and stifle. Walter has mild stifle effusion bilaterally, is reactive to palpation of his right stifle and is repeatedly tender to palpation of bilateral proximal to mid suspensory ligaments.
At a walk, no lameness noted. At a trot, in a straight line, Walter seems resistant to move forward and gait is short and choppy. When trotted on a lunge circle, foot fall of outside hind limb consistently short, more apparent on the right hind limb. When asked to canter on a lunge circle, Walter is resistant to load weight on his hind end for the upward transition. He repeatedly protests the trot to canter transition by bucking, and once he is cantering, he can only hold the gait for about half of a 20-meter circle before coming back to a trot.
Myofascial palpation: Walter has symmetric muscle mass with no appreciable muscle atrophy. He does not appear to have the characteristic dropped fetlocks commonly seen with suspensory desmitis. Walter has taut muscle bands and trigger points bilaterally in the omotransversarius, cervical serratus, trapezius and pectorals. Bilaterally, his gluteal fascia is taut and tender, his Superficial gluteal muscle, Biceps femoris muscle, lateral digital extensor muscle, long digital flexor muscle and deep digital flexor muscle are all diffusely taut and prominent bilaterally.
Diagnostic results: Radiographs of bilateral stifles (Photo 11-16) show suspect bilateral patellar lesions, small bilateral trochlear defects and suspect small bone cyst on the left proximal tibia. Ultrasound images of bilateral suspensory ligaments (Photo 5-10) show left hind diffuse remodelling and disruption of fiber pattern in zones 1B to 3C with a core lesion at zone 3C and right hind showed diffuse disruption of fiber pattern in zones 2A to 3C (per Dr. Brad Cumper, Figure 2)
Problem List
1- Repeatable painful response on palpation of bilateral rear suspensory ligaments at the origin and mid-body.
2- Mild bilateral stifle effusion with repeatable pain response on palpation of bilateral stifles, more pronounced on the right
3- Multiple prominent and taut muscles in the pelvic limb (gluteal fascia, superficial gluteal muscle, biceps femoris muscle, lateral digital extensor muscle, long digital flexor muscle and deep digital flexor muscle)
4- Palpable heat and multiple taut muscle bands and trigger points in the cervico-thoracic spine and chest (omotransversarius muscle, cervical serratus muscle, trapezius muscle and pectoral muscles)
Differential Diagnoses for Top Two Problems
-Vascular: While rare, decreased or compromised blood flow to bilateral hind limbs could be caused by partial aortic-iliac thrombosis, blood clots in other major vessels in the hind limbs or even deficits in micro-circulation, causing local ischemia and subsequent pain.
-Infectious: Bacteria or fungus can cause cellulitis, abscesses and possible septic arthritis which can all lead to pain/lameness.
-Neoplastic: Neoplasia that effects the brain or spinal cord can lead to neurologic related gait alterations. Although uncommon and not often bilateral, soft tissue or bone neoplasia can cause localized pain and subsequent lameness.
-Degenerative: DSLD, more recently renamed equine systemic proteoglycan accumulation (see reference #1), is most common in the rear suspensory ligaments but it can also affect ALL tendons and ligaments and associated connective tissue throughout the body, including the patellar ligaments.
-Iatrogenic: Adverse reaction to plasma transfusions as a foal could have led to possible breakdown of connective tissue
-Congenital: Friesian horses are a breed of warmblood known have imaging changes consistent with DSLD
-Auto-immune: Auto-immune diseases such as Equine fibromyalgia syndrome, immune- mediated neuritis or immune-mediated poly-arthritis could all lead to lameness and pain
-Traumatic: Separate injuries to both rear hind suspensory ligaments at different times could lead to bilateral hind suspensory ligament pain
-Endocrine/metabolic: Polysaccharide storage myopathy is an endocrine related disease that can lead to weakness/pain
-Myofascia: Starvation as a foal could have led to stunted growth and underdeveloped myofascia and connective tissue due to inadequate building blocks for appropriate muscle/ligament/tendon growth and development.
Putative/Definitive Diagnosis
I believe congenital/inherited DSLD, i.e. equine systemic proteoglycan accumulation is the putative diagnosis for Walter’s top two problems based on breed, age, multiple ligamentous/connective tissue structures affected, and a lack of supportive clinical signs related to other differential diagnoses.
Medical Decision Making
Beginning in April 2018, Walter received one month of weekly treatments, followed by two months of bi-weekly treatments, and he now receives monthly maintenance treatments. Cervical spine, shoulder, chest, back, hips and stifle were targeted during treatments. Walter’s treatments consist of a combination of dry needling and massage. Throughout his treatments, Walter did have days when he was very reactive to the dry needling. This is presumed to be a combination of flightiness due to his young age, as well as possible discomfort. On treatment days when Walter was less than enthused about dry needling, treatment was focused more on acupressure and massage.






Medical Acupuncture and Related Techniques
Seirin, J-type coated needles were used for each treatment. Treatments began with the use of No.3 (0.20)x30 mm needles in all locations. After the first session, a No.8(0.30)x40mm needle was inserted at Bai Hui at the beginning of each session. As Walter became more accustomed to the needles, No.3 (0.20)x30 mm needles were continued to be used for points in the distal limb/feet where as No.5 (0.25)x40mm needles were used in all other locations. Needles were left inserted for 20-30 minutes per session.
Dry needling points were chosen in order to provide neuro-modulation to all aspects of the nervous system and the myofascia.
Multiple points along the Gallbladder and Bladder channels stimulated the central nervous system and were also used regionally for trigger points and pain. The autonomic nervous system was specifically targeted using ST 36, GV 20, BL 40 and Bai Hui. The peripheral nervous system and myofascial planes were targeted as outlined below:
-Neck: TH 16, LU 1, LU 7, GV 20, LI 16, GB 20
-Shoulder: TH 14, TH 15, SI 9, GB 21
-Chest/pectoral: LU 1
-Lumbo-sacral region: BL 20, BL 21, BL 22, BL 23, BL 24, BL25, BL, 26, BL 27, BL 28, BL 29, BL 30, BL 40, GV 4
-Stifle: Medial Xiyan, ST 36, ST 35, ST 34, SP 9, SP 10, GB 34, GB 39
-Hip: GB 29, GB 30, BL 54
-TH 1 and LR 1 were used to neuromodulate the distal pelvic limb
Outcomes, Discussion
Over Walter’s 5 months of treatment, significant changes were seen in his attitude and overall comfort level. Licking, chewing and yawning were often observed during treatments which indicated a sense of relaxation. I think it is important to remember that when treating one injury aggressively, other parts of the body are implemented. I believe that Walter’s aggressive shoeing for his suspensory injuries caused secondary pain and body soreness to muscles in his proximal pelvic limb and lumbo-sacral region due to prolonged heel elevation and stall rest.
Overall, there was a small improvement in lameness in the hind end, but it is possible that if his DSLD is also affecting multiple other connective tissue structures in the body, he may never be 100% sound. I believe that maintenance acupuncture treatments may help Walter to be comfortable as a riding horse at a walk/trot level, but he may never be sound in the canter. If tolerated by patient, electro-acupuncture may increase response to treatment and duration of treatment effects.
References
1. Degenerative suspensory ligament desmitis- A new reality. Halper J, Khan A, Mueller POE. Pakistan Veterinary Journal. 2011 Nov; 31(1) 1-8
2. Degenerative suspensory ligament desmitis as a systemic disorder characterized by proteoglycan accumulation. Halper J et al. BMC Veterinary Research. 2006 April; 2(12)